
Claire Helm
Senior Analysis Manager
NHS Providers
Introduction
Since launching our inclusive leadership series in September, the focus of the conversation has rightly centred on addressing racism in the NHS, confronting white privilege and discussing improvements and shortcomings in the equality, diversity and inclusion agenda.
Here we broaden our focus by exploring gender diversity and the gender pay gap at trust board level.
Encouragingly, our research shows that gender diversity across trust boards is improving, albeit slowly. Similarly, salary data shows the gender pay gap is narrowing. However, variation across director roles persists, most likely resulting from the gender imbalance in the medical, nursing, finance and HR professions.
There is also statistically significant variation in pay across roles. The variation is characterised in two ways. Firstly, salaries for predominantly female board roles are lower than those for board roles that are predominantly male. Secondly, male executive directors across the majority of board roles are paid more than their female counterparts.
The gender pay gap is a symptom of wider systemic and cultural issues. Actions are currently being taken across the NHS to seek to address the gap include role modelling and the use of positive discrimination in recruiting. It is clear, however, that there is not simply one formula or toolkit which will improve diversity and reduce the gender pay gap of NHS boards overnight. Instead, strategies to improve diversity within the pool of future and aspiring executive directors need to be tailored across different professions, accounting for the variety of clinical and non-clinical career paths taken before stepping into NHS leadership roles.
The gender pay gap in the NHS
The gender pay gap in the UK has been declining slowly over the last decade. It has fallen by approximately a quarter among full-time employees and by just over one-fifth among all employees. In April 2020, for full-time employees, the median gender pay gap was 7.4% in favour of men - down from 9.0% in April 2019. The gender pay gap increases to 15.5% for part-time workers in favour of men. The Office for National Statistics also found that, although COVID-19 has had a substantial impact on labour market activity, including the introduction of the furlough scheme and increased levels of unemployment, it appears to have had little impact on the gender pay gap.
Nuffield Trust analysis from May 2019 showed a median gender pay gap of 8.6% across the NHS, favouring male employees. The findings showed that the gender pay gap for the 88% of the workforce who fall within the Agenda for Change pay structure was 3.9% in favour of women. This is largely driven by occupational segregation and the largely female composition of the nursing and support workforce. In fact, 77% of the total NHS workforce is female.
However, the gender pay gap within the highest pay bands across trusts is in favour of men. These bands, which apply to the medical workforce and very senior managers (VSMs), consist of a disproportionately high number of men, with the Nuffield research showing a gender pay gap of 47%.
Gender representation and remuneration at board level
Each year NHS Providers carries out a benchmarking survey capturing the remuneration details of executive directors, a subset of very senior managers (VSMs), who sit on NHS trust and foundation trust boards. The latest survey looked at 1,049 roles across 148 trusts - accounting for 66% of the provider sector.
50% of executive directors are female and 50% are male – a welcome development over the past few years. This is significantly higher than the 33% female make up of FTSE 100 boards. However, when unpicking the data from trusts, there is noticeable variation in the gender split between roles, particularly with finance directors and clinical roles such as nursing and medical directors. Differential pay structures exist across several of the different roles, for example finance and medical directors who are predominantly male are, on average, paid more overall than nursing, workforce and HR roles which are predominantly female.
Executive director roles by gender
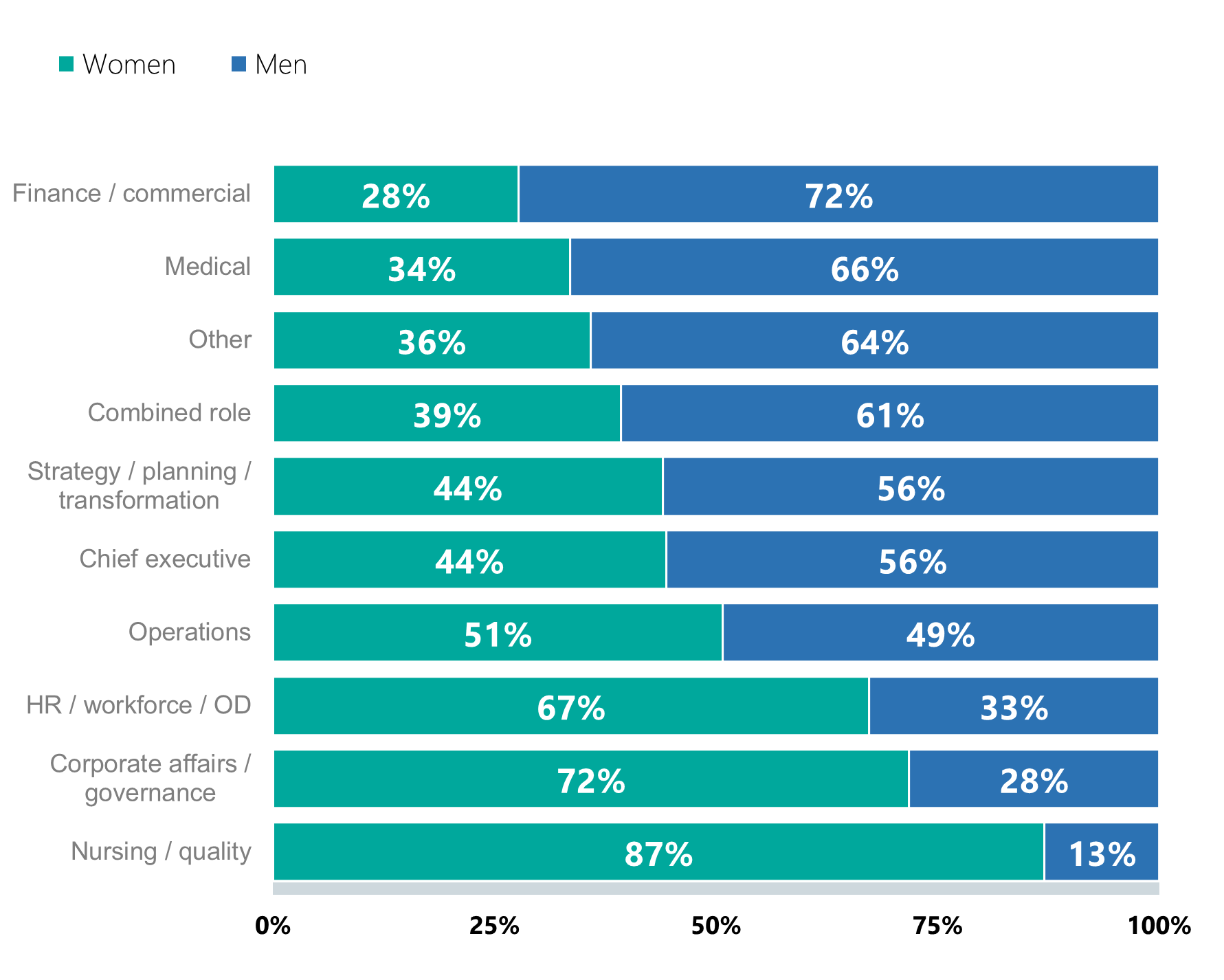
The gender imbalance among nursing directors reflects the fact that 89% of the nursing workforce is female. However, the medical workforce gender split is 46% female and 54% male, making the underrepresentation of women in medical director roles a particular concern. Furthermore, an independent review led by Professor Dame Jane Dacre recently reported a 17% gender pay gap between women and men in the medical workforce overall.
The gender pay gap across all executive director roles is around 10% - on average, women at board level are paid £13,250 less per annum than their male counterparts. Encouragingly, in a similar vein to the wider labour market, our annual survey shows the gender pay gap is shrinking - down from 12% in 2017 when the difference was £15,000.
Overall, the gender pay gap for NHS executive directors is therefore practically in line with national figures – a 9.8% average gap for chief executives and senior officers across the UK. The gap favoured men across the majority of board roles, with the exception of nursing/quality directors and those in the ‘other’ category. The average salary for directors of operations was equal across women and men, following a similar pattern to the gender split for the role itself - perhaps reflecting the fact that there isn’t a single pathway or 'access' role for this particular profession.
Closing the gap
While this information is illuminating the most important thing it highlights is the need to take action. So, how do we close this gap? As the largest employer in the UK, the NHS must play a leading role in addressing the gender pay gap. Since April 2018, all organisations with 250 or more employees have been required, by law, to report median and mean gender pay gap figures to the Government Equalities Office and the Equality and Human Rights Commission. It is hard to know if the introduction of these requirements has contributed to the narrowing of the gap in the past few years but undoubtedly the additional transparency around pay helps trust boards benchmark and track their performance.
Our data shows that racial and gender diversity and pay gaps vary by board role. There are likely to be different barriers depending on race and gender which are also intersected by whether a director has followed a medical, nursing or non-clinical route. The variety of career paths to board level and chief executive need to be mapped and the barriers to progression for people of colour and women fully understood. By focusing on the diversity of distinct pipelines of future leaders we will help boards become more diverse and eradicate the pay gap. This needs to sit alongside more immediate programmes of action to identify and reduce existing levels of inequality.
Boards and the inclusion agenda
With the increased focus on race and the inclusion agenda this year, NHS leaders are closely examining what they can do collectively and as individuals to support diversity across their organisations. And, although not tackled in this piece, we know that the intersection of different protected characteristics – such as race and gender – has a compounding negative impact.
Increased flexible working, embedding effective staff networks that feed into decision making processes, changes to recruitment strategies, equality and diversity training, reverse-mentoring, coaching, inclusion cafes and expanding aspiring leadership programmes are just a few of the actions trusts are taking to improve diversity and inclusivity within their organisations. But we know more needs to be done.
Although progress is slow, gender diversity across NHS leadership is heading in the right direction. The power to speed up the pace of change sits firmly with trust boards themselves – delivering it is a central pillar of good leadership.
We know there are many benefits to organisations that are diverse – it is better for patients, improves staff wellbeing and productivity, and helps staff feel valued. The NHS must also reflect the diversity of the populations it serves. Embedding inclusive leadership and improving diversity at board level will only help amplify the benefits to patients and staff.