Mental health services are continuing to experience rising demand that matches and, in many cases, exceeds available capacity in both adult and children and young people’s services. Bed occupancy rates for inpatient mental health services regularly exceed the 85% level recommended to maintain patient safety standards, highlighting the significant pressure the system is under. Adult and children and young persons mental health services are seeing similar or greater increases to those observed in acute and urgent and emergency care.
Recent NHS statistics on mental health performance further illustrate the demand challenge for mental health trusts. In November 2018 (NHS England, 2019):
- The number of people in contact with NHS funded secondary mental health, learning disabilities and autism services increased by 4.1% to 1,310,985 (51,496 more people) compared to the average number of people contacting per month in the past year.
- Of these 1,310,985 individuals, 78% were in contact with adult mental health services, 17% were in contact with children and young people’s mental health services and 8% were in contact with learning disability and autism mental health services.
- The number of new NHS funded secondary mental health, learning disabilities and autism services referrals increased by 12.4% to 320,349 (35,343 more people) compared to the average number of new referrals per month between in the past year.
- There were 710 active out of area placements, an increase of 5.2% compared to the previous year.
- The number of children and young people starting treatment for an eating disorder has increased by 4.9% compared to the same time last year.
- There were 144,722 referrals to talking therapies. Demand for IAPT services is increasing. New referrals increased by 3.9% from 2016/17 to 2017/18. Meanwhile, referrals that entered treatment increased by 4.5% over the same period.
There were 710 active out of area placements, an increase of 5.2% compared to the previous year.
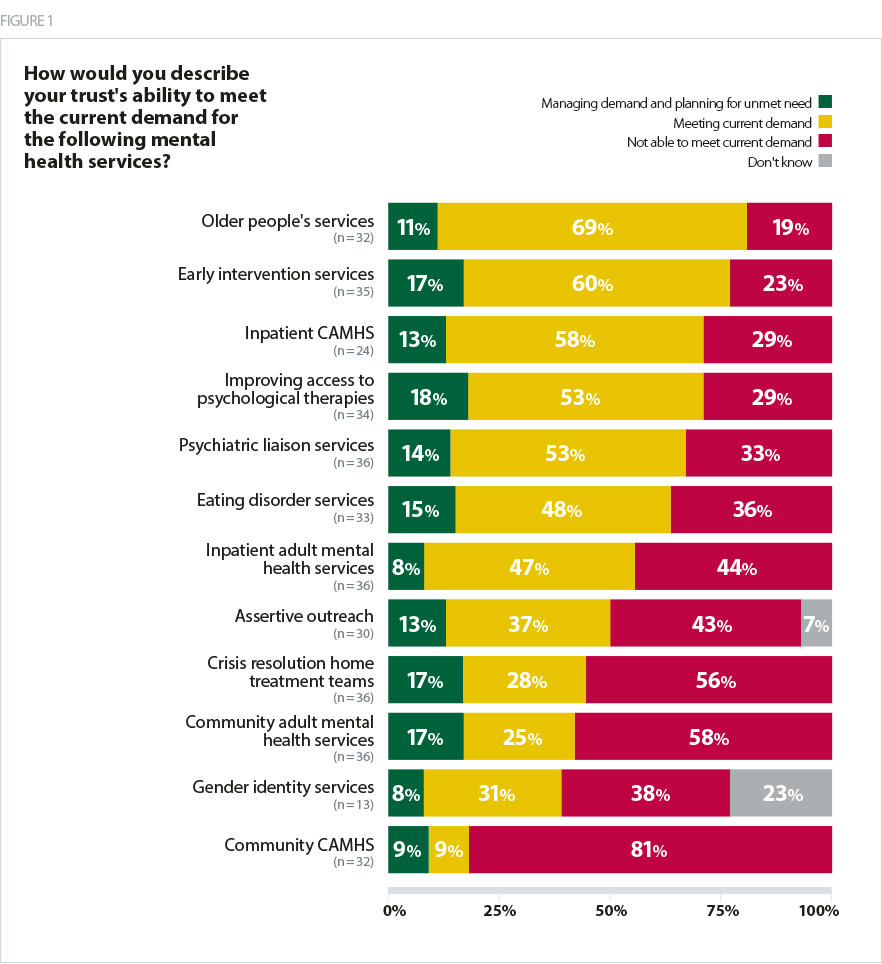
We asked mental health leaders about the drivers and levels of demand their trusts were experiencing across the range of services that they provide. Encouragingly, as shown in Figure 1, trusts are meeting current demand for many services, and in some areas are putting plans in place to fulfil unmet need. The services that trusts are equipped to better manage demand include: older people’s services, early intervention services, inpatient child and adolescent mental health services (CAMHS), and talking therapies (IAPTs). And 18% of leaders said they were making plans to meet unmet need for IAPT– the highest proportion across all services.
Significant pressures on core community services
However, there are a number of areas in which trusts are struggling to meet current levels of demand. An overwhelming majority (81%) of trust leaders said they are not able to meet current demand for community CAMHS and 58% said the same for adult community mental health services. In relation to overall community provision, 85% disagreed or strongly disagreed with the statement that there are adequate mental health community services to meet local needs. That said, 39% of leaders were positive about the direction of travel in community services and agreed or strongly agreed that services in their local area were improving.
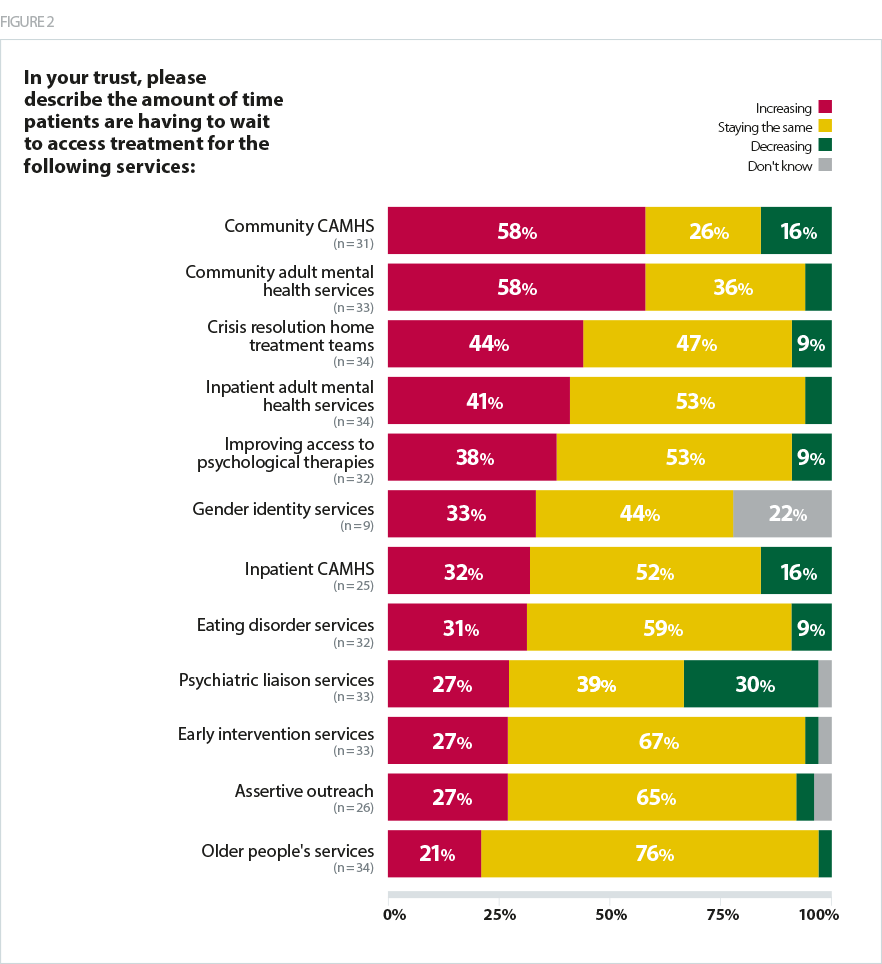
We also asked trusts about the services they provide, including questions on access, changes to and quality of services. As shown in Figure 2, a small number of trusts across the country felt that the amount of time people are waiting to access services such as psychiatric liaison, community CAMHS and inpatient CAMHS is decreasing. However, far more trusts reported that waiting times were increasing:
- 58% increase in waiting times for community CAMHS
- 58% increase in waiting times for community adult mental health services
- 44% increase in waiting times for crisis resolution home treatment
It is encouraging that community based mental health care is a key focus of the NHS long term plan, given mental health trust leaders have highlighted that meeting current demand for services in the community is a particular challenge and waiting times for these services are also increasing. However, there remains a lack of detail on how key initiatives proposed in the plan to drive this agenda, such as the new integrated models of primary and community mental healthcare and the mental health support teams, will be delivered in practice given the current pressures on the sector. This will need to be addressed in the upcoming workforce and implementation plans due out later this year.
Challenges facing inpatient services
In our survey, trust leaders also pointed to growing pressures on inpatient services for adults – where demand for and access to beds is particularly challenging. 52% of mental health leaders disagreed or strongly disagreed with the statement that there are enough inpatient mental health beds in their trust/local area. However, pressure does not only come from demand and access. Trust leaders also report an increase in the severity of service users’ conditions, which is partly attributable to people having to wait longer to access the services they need. This can result in them needing more specialist, longer-term care.
When no inpatient beds are available within an appropriate timeframe, one solution is to find beds 'out of area' to ensure service users receive the care they need as quickly as possible. This is not an ideal solution. Placing a patient out of area impacts the overall quality of care, particularly in terms of service user experience, can delay recovery through disconnection from family, carers and support networks, and fragment continuity of care. It is also more expensive.
The level of out of area placements (OAPs) is an important signal of the level of pressure in-patient services are under; OAPs have significantly risen in recent years, as our survey shows:
- 70% of leaders said they had acute inpatient out of area placements
- 63% said they had CAMHS tier 4 out of area placements
- 58% said they had rehabilitation out of area placements.
In our survey, trust leaders also pointed to growing pressures on inpatient services for adults – where demand for and access to beds is particularly challenging.
In our survey, alongside ongoing increases in demand, trusts identified a number of factors contributing to their reliance on OAPs including:
- Increased length of stay
- increasing severity of inpatients’ conditions means they need to stay longer
- Investment
- a low bed base across the country as a whole
- low levels of investment from clinical commissioning groups (CCGs)
- use of block contracts to pay for services
- Type of provision
- lack of specialist provision
- insufficient community based services
- accommodating changes to the use of Section 136 of the Mental Health Act
Barriers to reducing OAPs include the high use of section 136 and the pressure on places of safety given recent changes to legislation and reduction in assessment time from 72 hour to 24 hour. The reduction in the use of custody is positive but did not plan for the subsequent increase in capacity.
Mental health trust
These findings underscore the need for an approach towards policy and funding for the sector that balances delivering on the ambitions for greater prevention, early intervention and community based care, whilst ensuring continued funding for, and access to, inpatient services that people with severe and enduring mental health conditions particularly rely on.
The impact of wider system pressures
We know that the nature of demand across local systems is not straightforward with increasing numbers of people having complex needs that can require a response from multiple services. 88% of mental health trust leaders agreed or strongly agreed that pressures in the wider system have a knock-on effect and increase demand for mental health services in other settings.
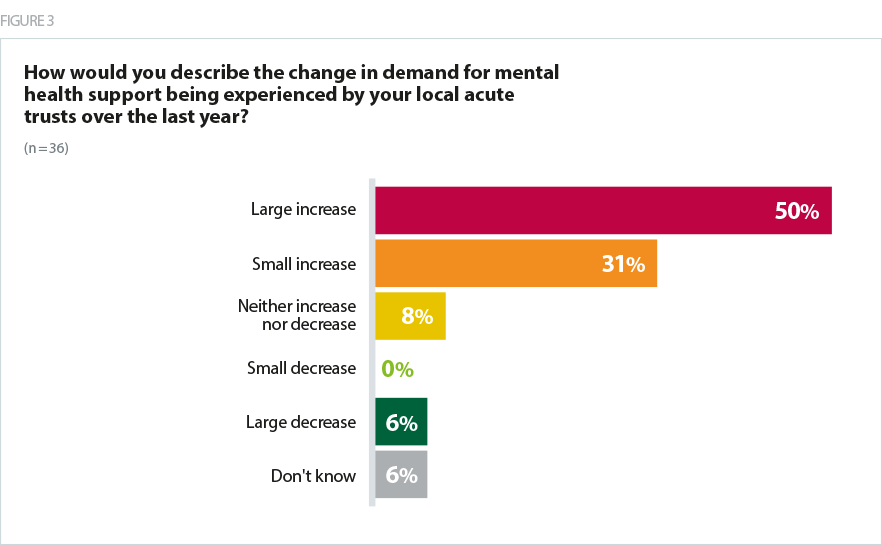
As shown in Figure 3, 81% of trusts leaders said that their local acute trusts had experienced a large increase (50%) or a small increase (31%) to the demand for mental health support over the last year.
For ambulance services, 39% of mental health trust leaders said their ambulance trust is able to respond effectively to support people experiencing mental health issues;,23% said they were not able to respond effectively and the remaining responses said they were 'neither able nor not able' or they did not know.
Our findings relating to ambulance and hospital services underscore the need for mental health expertise in all parts of the system. The long term plan makes welcome commitments to build the mental health response competency of ambulance staff and to make mental health liaison services available in all acute hospital A&E departments that – if adequately resourced – should help to build capacity.
Trusts also highlighted how changes to the law were impacting on capacity. More than two thirds (69%) of trusts leaders said that changes in how services users are managed under section 136 of the Mental Health Act (MHA) have resulted in trusts allocating increased resources to implement these. The main changes to section 136 include a reduction in the maximum period of detention from 72 hours to 24 hours before being admitted to an inpatient setting, under 18s no longer being allowed to be taken to a police cell and adults only being taken to a police cell under certain circumstances. Police are also required to consult a mental health professional before applying a section 136 where possible. These changes put substantial additional pressure on inpatient capacity.
Prioritising early access to a health professional in a suitable environment is vital to improving the treatment of those experiencing mental health crises. However, the availability of places of safety and appropriate staff remain key issues that need to be addressed. Sufficient numbers of approved mental health practitioners and alternative places of safety need to be commissioned and appropriately funded. Commissioning and funding adequate numbers of mental health beds and alternative services across the country is also essential to combat out of areas placements and difficulties in managing flow of service users – particularly in urgent cases – arising from changes to how patients are managed under section 136 of the Mental Health Act.
More than two thirds (69%) of trusts leaders said that changes in how services users are managed under section 136 of the Mental Health Act (MHA) have resulted in trusts allocating increased resources to implement these.
The drivers of demand
The drivers of demand for mental health services are complex and often multifaceted. Across health and care we focus heavily on the pressures that hospital services face in winter – arising from the combination of cold weather, flu, an increasingly frail population, a stretched workforce and an inability to discharge patients. Nearly half of trusts leaders (48%) agreed with the statement that ‘demand for mental health services increases over the winter months’, showing that the seasonal peaks in demand for care are not unique to physical health.
However, whilst winter pressures can increase demand for urgent and emergency care, mental health has other drivers of demand which have a year round impact. A significant number of mental health trust leaders stressed the impact of wider socioeconomics factors on demand for mental health services in their responses to our survey.
Figure 4 shows the external factors that trust leaders identified as having an impact on increasing demand:
- 92% said changes to benefits/universal credit – with 63% saying the impact was high, making it the most significant factor
- 98% said financial hardship
- 97% said housing
- 97% said loneliness and isolation
- 91% said cuts to local services
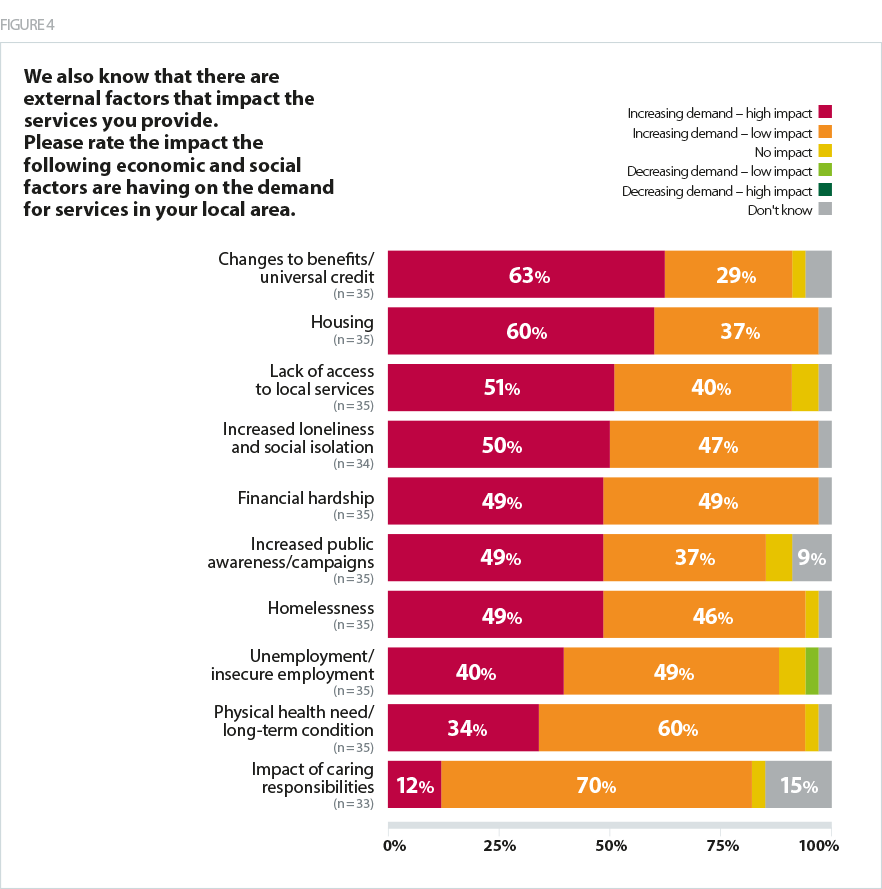
Trusts leaders told us that they are very concerned about the impact of growing social and economic hardship in their local communities. In particular they pointed to changes to benefits and the effects of financial hardship, homelessness, and substance and alcohol misuse playing a growing role in the nature and volume of presentations to mental health services.
Main impact is from high and increasing levels of deprivation in this post-industrial area - so the main determinant is economic. Locally, substance misuse is rising rapidly and funding of provision for care and treatment via local authorities has more than halved - the consequences were and are self-evident.
Mental health trust
Cuts to substance misuse services, at a time when the use of new synthetic drugs such as spice and monkey dust has increased, was singled out in particular as a key local factor affecting demand.
The Local Government Association estimates that between 2010 and 2020, councils will have lost 60p out of every £1 the Government had provided for services (Local Government Association 2018). Mental health trust leaders have said such deep cuts to local authority and voluntary sector budgets have meant the availability of vital services has dramatically reduced.
Cuts to local authority and voluntary sector budgets have dramatically reduced the availability of services - The NHS is the only one still "open"!
Mental health trust
Respondents also stated increasing deprivation and financial hardship, resulting from changes to the benefits system in some cases, is having a serious impact on driving demand for mental health services. Universal credit was specifically named as a policy which was impacting on a number of those presenting to mental health services.
Case study 1: Denise
Denise (49), who has bipolar disorder, about her experience of the work capability assessment (WCA) process.
"I’ve been affected by mental illness since I was 16 years old but wasn’t diagnosed with bipolar disorder until 1992 when I was 25. Despite my mental health condition I took medication for it and I worked as a mental health nurse all my life until 2011, when I became physically unwell with spinal problems and was forced to leave my job.
That was the first time I had ever had to apply for benefits and I found the whole process a huge source of anxiety. I felt lost and if I ever called the Department for Work and Pensions (DWP) to ask anything in relation to my employment support allowance (ESA) claim they would be so rude and uncooperative on the phone. I have found it extremely stressful to the point of a relapse in my mental health when I had to chase numerous professionals for supportive evidence to confirm that my mental health can prevent me from working. My mental health really deteriorated when I was forced to give up work. I think it was a direct response to the loss of income, social contact and vocational enjoyment and my personal sense of purpose.
My first work capability assessment in 2011 was really intimidating and provoked an enormous amount of anxiety in me. The assessor seemed to contradict everything I said and it was like she was misleading me so I would answer in a certain way. She had no compassion or even any understanding of my mental illness. She just asked a lot of irrelevant questions and it felt like she was on a strict time limit just firing out the questions to get it over with as quickly as possible.
As I have bipolar disorder my mood fluctuates and on that day I was feeling relatively well but on other days I really struggle and don’t even get out of bed. Afterwards I was found fit for work and I was beside myself with worry. I went to my local mental health support service and they gave me advice on how to appeal. During that process my circumstances changed and I moved abroad for a while so I abandoned it.
When I returned to England in 2013 I had go through the process again. Finding all the evidence for a second time and having another assessment was really stressful. This time round I was feeling so depressed on the day of the assessment that I really didn’t care what happened. They must have picked up on this. Nothing had actually changed in my circumstances since my last assessment but this time I had a totally different outcome and was found unfit for work and put in the support group.
I thought I was safe and wouldn’t have to worry about having to go through the assessment again but in the last month I have been made to re-apply for ESA and gather all the evidence from my doctor and other medical professionals yet again. I can’t tell you how stressful it is.
I think the whole process is cruel. I have to wait for four weeks for a decision and I’ll have sleepless nights until then. My security has been taken away. I also get some housing benefit but it isn’t enough and part of my ESA pays my rent. Without my ESA I could become homeless. Going through the work compatibility assessment process is the biggest source of worry in my life and it’s in the lap of the gods as to what happens to me next. I feel powerless."
While the link between poor mental health and poverty is understood in terms of driving up demand, it also impacts on the capacity of the workforce. Our findings suggest that community mental health staff in particular are spending increasing amounts of time supporting service users to navigate the benefits system, as well as supporting general issues associated with hardship including deterioration in wellbeing.
Housing and homelessness were also cited as increasing demand for services. There are a number of positive examples of mental health trusts working to overcome challenges around housing, including working in partnership with primary care and the third sector to provide supported housing and residential care with housing associations.
Case study 2: South West Yorkshire Partnership NHS Foundation Trust providing housing support services
Chelsea Huskins works for South West Yorkshire Partnership NHS Foundation Trust as a housing support co-ordinator. She explains:
"Sometimes, it isn’t people’s health needs that keep them in hospital. Problems with finding suitable accommodation for people who have had a long stay on a mental health inpatient ward can mean that they spend extra time in hospital which could have been avoided.
I work as a housing support co-ordinator across four wards in Wakefield, which means that I support people with mental health conditions to move back into suitable accommodation following a stay in hospital. When people with housing needs are admitted they are referred to me. They might have been homeless when they came to us, or staying with family members who they’re unable to return to.
I explore different options with housing authorities and landlords to make sure that accommodation is in place so that when a person is well enough to be discharged, they’re not kept in hospital for any longer than they need to be.
In just under a year I’ve had 76 referrals. I’m still in the process of supporting a couple of people, but apart from that I’ve found suitable accommodation for everyone.
Before my role was in place, lots of people would have to support someone to find accommodation. It meant that work was sometimes duplicated or missed, but now people can just come to me and all the work can be co-ordinated by one person. It’s also good to have someone who has housing knowledge and contacts. Quite often, service users will be more willing to open up to me about their goals and needs as they don’t see me as part of the nursing team.
With the help of my role, people are reaching their potential and living well in their communities, and are able to return home as soon as possible to continue their recovery."
The impact of pressures on quality
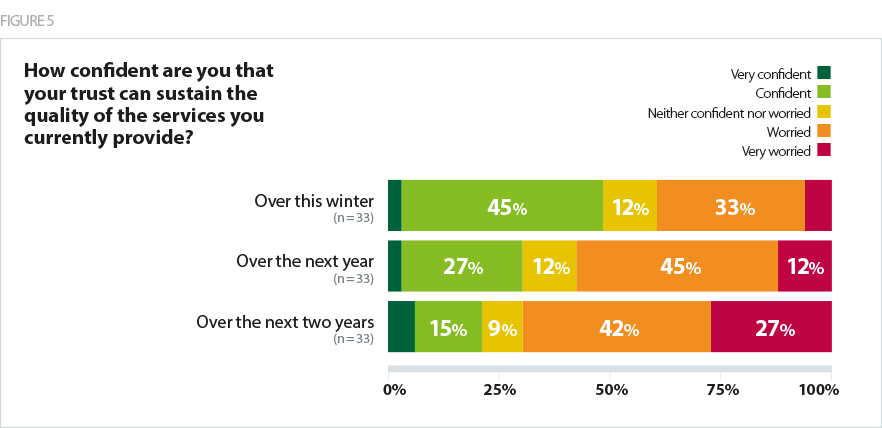
When asked about the quality of services, around half of trusts felt confident or very confident that they can sustain the quality of service they currently provide this winter. As Figure 5 shows, this trend shifts when looking at confidence over the next year and then over the next two years. In fact, 69% of mental health leaders are worried or very worried about being able to maintain the current quality of service over the next two years.
Demand for services is a complex issue. It is both a reason for, and result of, the care deficit permeating mental health services. If we are to address this we need to see:
- National policy moving in the same direction with increased support for both mental health and public health – local authority services are a key element in both meeting current need and preventing future demand
- Realism about demand and what is needed to meet it, given that raised awareness of mental health issues and wider socio-economic factors will increase demand for services
- Better demand and capacity planning with inputs from both trusts, commissioners and the national bodies