In this section, we explore the possible costs of recovering performance in:
- elective care, against the 18-week target
- accident and emergency, against the four-hour standard
- delayed transfers of care (DTOCs)
- mental health, community services and ambulances, by restoring the workforce.
Recovering elective care performance
Table 3
There has been a sustained decline in performance against the 18-week referral to treatment standard over the past three years:
- across the NHS trust and foundation trust sector 86.8%of patients were treated within 18 weeks of referral at March 2018. This was the worst performance against the 92% standard since 2011
- the likely number of patients on the waiting list was 4.1 million – although a precise figure cannot be given because a small number of trusts do not report against this standard. This is as high as in August 2007, (Findlay R., June 2018) when the national waiting list was first reported
- the number of people waiting more than a year for an operation nationally increased from 1,513 to 2,647 between March 2017 and March 2018.
The increasing likelihood of patients waiting longer than 18 weeks for a planned operation is one of the most visible symptoms to the public of the financial pressure on the NHS.
The main cause was the impact of an unplanned-for rise in emergency activity, which diverted inpatient ward and operating theatre capacity away from elective work. There were also clear signals from national leaders that, where there was not enough capacity, the priority should be to meet the need for emergency care.
There has been a sustained decline in performance against the 18-week referral to treatment standard over the past three years
The outcome has been bad for patients, who have suffered from lengthening waiting times and last-minute cancellations. For provider trusts, it led to a combined shortfall in expected income of £505m in 2017/18. There were 300,000 fewer elective operations carried out than providers were planning for – indeed the overall number of procedures in 2017/18 was around 60,000 less than 2016/17.
To recover this position, analysis by Rob Findlay, a waiting times expert, indicates that the service will need to reduce the overall waiting list to no more than 3.5 million in order to hit the 18 week target. That means the service will have to both reduce the backlog by about 600,000, and increase the number of operations carried out annually by 170,000 to stop it growing again.
This research concludes that, at a conservative estimate, the NHS needs to spend £1.8bn on clearing the waiting list and a recurrent £350m extra per year to keep up with the additional demand.
Restoring acute inpatient capacity
Table 4
The A&E four-hour standard is a barometer of a local system’s overall ability to cope with demand. Trusts struggling to meet the standard is an indication of a lack of general capacity within the wider system, including the hospital.
In quarter four of 2017/18 acute trusts admitted or discharged 82.5% of accident and emergency patients with four hours, against the target of 95%. For major A&E departments (known as type 1) performance was 76.8%. The NHS as a whole last met the 95% target for all types in July 2015.
Our analysis has used acute inpatient capacity as a proxy for overall system capacity, and explores how much extra capacity would be needed to recover performance on the four-hour A&E standard. Where new funding can be used to bolster capacity, it should be up to local systems to decide what should be expanded, and leaders may decide to place the investment into primary care, the community sector or social care. All will have costs attached.
In quarter four of 2017/18 acute trusts admitted or discharged 82.5% of accident and emergency patients with four hours, against the target of 95%. For major A&E departments (known as type 1) performance was 76.8%.
Nevertheless, it is certain that, with systems as they were configured in winter 2017/18, with average length of stay at five days and admissions at 6.3 million (NHS Digital, 2017), the NHS did not have enough acute capacity to be able to safely meet demand.
Admissions in 2017/18 were up 3.5% on 2016/17, and 2.2% more than planned (NHS Improvement, 2018). Despite this, the average number of general and acute beds open fell by around 500 year on year. The total number of acute beds has fallen by 6.3% since 2010-11, and we note that the 2018/19 planning round has revealed further planned reductions (NHS Improvement, 2018). This will continue – with predictable effects on performance and patient experience – for as long as system capacity remains out of step with rising demand.
In addition to its impact on headline A&E performance, the lack of surplus capacity in hospitals led last winter to a sharp rise in mixed sex accommodation breaches (NHS Providers, 2018), and will also make it harder to control rates of healthcare acquired infections.
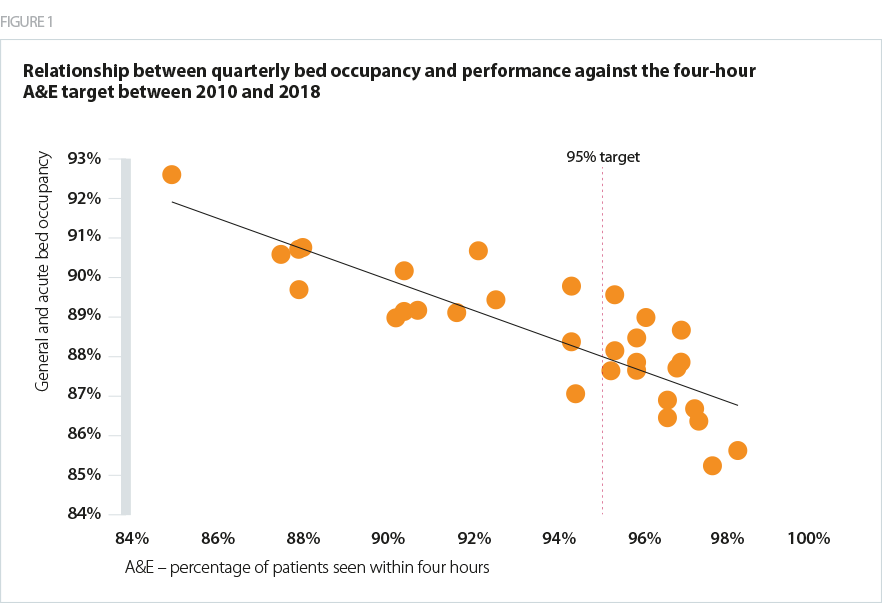
There is no single commonly agreed optimum occupancy level for acute inpatient beds – figures ranging from 85%t to 92% are often cited.
There is a strong correlation between the NHS meeting the four-hour target and occupancy levels of 88% and lower (figure 1). Since quarter 2 2010/11, the NHS has been unable to meet the four-hour target with occupancy levels over 90%.
According to winter sitrep data, there were on average 98,375 total acute inpatient beds available during February, including escalation beds. Occupancy was on average 95%. This would put the average number of inpatients at 93,456.
To get back to 88% occupancy, the NHS in England would have needed an additional 7,825 inpatient beds in February 2017/18. To achieve 85% occupancy – the figure used by Care Quality Commission (CQC) in its most recent State of care (CQC, 2017) report, 11,573 extra beds would have been needed.
This estimate is conservative: in addition to acute physical health beds, that a serious investment is needed in mental health inpatient provision.
We cannot rely on further reductions in delayed transfers of care to boost capacity. While we made good progress over 2017/18, the improvement was not of the order needed to free up the equivalent of 2,000-3,000 hospital beds nationally as originally required (NHS England, 2017). Efforts of this type – for example this year focusing on ’super stranded’ patients – will continue but it is prudent, based on past experience, to be sceptical that initiatives such as this will lead to a material increase in hospital inpatient capacity quickly.
Using excess bed days – the average cost of a patient sitting in a bed after their treatment has ended – we can estimate the annual cost of this extra provision would be at least £894m. However, as stated earlier, there are a variety of ways different systems could choose to spend that sum depending on local needs.
To get back to 88% occupancy, the NHS in England would have needed an additional 7,825 inpatient beds in February 2017/18.
Funding to aid social care and NHS joint working
Table 5
Social care and the NHS are interdependent. Social care is a vital public service in its own right which, for the sake of people who rely on it, needs to be put on a sustainable footing.
But the prospects for social care are also essential to the success of any long term plan for the NHS. The precarious position of social care represents a general risk for trusts, but there is one diminishing funding stream which represents a specific threat: the non-recurrent money allocated to social care in the 2017 spring budget.
The cash was worth £1,010m in 2017/18, falling to £674m in 2018/19 and £337m in 2019/20. It then disappears altogether. When it was introduced, councils were given an explicit mandate to work with local NHS leaders on how their share should be spent to support social care and relieve pressure on the NHS. The budget required councils to: fund care packages for more people; support social care providers; and relieve pressure on the NHS locally. It is not known how much of the £1bn in 2017/18 was specifically spent on schemes to reduced delayed transfers, although any funding not spent directly on reducing delayed transfers will of course have indirectly benefited the NHS by shoring up social care.
The investment does appear to have helped reverse an entrenched trend of steep increases in the rate of delayed transfers of care.
The precarious position of social care represents a general risk for trusts, but there is one diminishing funding stream which represents a specific threat: the non-recurrent money allocated to social care in the 2017 spring budget.
In 2016/17 the rate of DTOCs increased by 25% year on year to more than 2.25 million delayed days. In 2017/18, following the first year of the new DTOC money, the overall number of delayed days was just under 2 million – returning the system almost to 2015/16 levels (NHS Providers, May 2018).
Across England, this translated into 1,600 more beds being made available daily for patients. This was short of the 2,000-3,000 hoped for but a meaningful improvement (NHS England, 2017).
More than two thirds of NHS trusts and local authorities have reduced the number of delayed days over the past year, suggesting the new money paid for interventions which worked in most places. The rise in successful joint working between councils and the NHS is encouraging, but will not be sustained if investment is not continued.
The success of 2017/18 must continue to be built on. The dedicated funding for social care, with its explicit mandate to reduce pressure on the NHS, should in 2019/20 be brought back up to £1,010m and then be maintained at that level. This means an extra cost of £673m in 2019/20 and £1,010 in each of 2020/21 and 2021/22. The latter two figures may not be necessary if the public funding for social care in those years changes as a result of the forthcoming comprehensive spending review.
Table 6: Restoring mental health capacity
Mental health mirrors the pressures physical health has seen in recent years. Inpatient capacity has gone down, appropriate community capacity has not been put in place, the workforce has fallen and demand has gone up.
However the amount of mainstream capacity provided outside the NHS trust sector, the lack of historical performance and activity data all make it harder to calculate the gap between current performance and what should be expected.
Unlike with A&E, it is not possible to point to a time when mental health standards were being met and discuss how the service may return to that level of performance. The prime minister’s funding announcement acknowledges that mental health has not been seen as being as important as physical health in the past, and pledges more money for the sector to rectify this.
For the purposes of opening a discussion about how much the mental health sector has been squeezed since 2010, we have chosen the nursing workforce as a proxy.
Compared with August 2010, the overall NHS mental health nursing workforce had fallen by 12.1% by March 2018, based on an annualised monthly average to remove seasonal variation.
The prime minister’s funding announcement acknowledges that mental health has not been seen as being as important as physical health in the past, and pledges more money for the sector to rectify this.
Head of Policy and Strategytweet this
Figure 2
Within those figures, there has been a fall of 25% for inpatient services – around 6,000 nurses – and an increase in community mental health nurse numbers of just over 1,500. The total shortfall compared with 2010 is 4,577.
To give an indication of the cost of recovering capacity in the mental health sector, we therefore believe it is reasonable to assume that as a minimum there should be a return to the overall workforce levels seen in 2010, before the funding squeeze began. We have not addressed the costs of expanding mental health services to meet patient need and demand, but have only considered the costs of recovery – this has to be considered in the context of financial and workforce underpinnings in the 10 year plan.
Based on average salaries and the calculation that the NHS needs another 4,577 mental health nurses to return to the numbers employed in 2010, it would cost £146m to return to that position. This works on the assumption that there are staff available to be recruited – in reality the current workforce shortages mean that filling these gaps will take time, and additional costs would be required to develop the required workforce.
Table 7: Restoring capacity in the community sector
We know that community services are also stretched, driven by the same underfunding and staff shortages and similar changes in demographics and acuity (NHS Providers, 2018).
As with mental health, there is an absence of activity data showing the changes in demand in this sector. Here we have used the nursing workforce as an indicator of how far the sector has been cut in recent years, and what the costs might be of restoring it. We have not addressed the costs of expanding community services in the way anticipated in the Five year forward view, and this again will need to be properly explored in the 10 year plan.
The community sector has seen significant structural change since 2010: in particular the impact of the transforming community services programme, which resulted in some services being transferred to community interest companies or private providers. It is difficult to strip out the impact of this on the overall workforce numbers.
Based on an annualised monthly average to remove seasonal variation, there were 5,885 fewer registered nurses (including health visitors) working in community health services than in May 2010.
Figure 3
After a sharp decline in the early years of the austerity period, there was a rise between 2012 and 2016 driven mainly – though not solely – by a rise in health visitor recruitment. In March 2018 there were 295 fewer health visitors than in May 2010 – however at their October 2015 peak there were more than 2,000 more health visitors than there are today. This volatility may have partly been caused by government’s introduction and later abolition of a recruitment target for health visitors.
The annual pay costs to increase the nursing workforce across NHS community health services by 5,885 would be approximately £189m.
Ambulance sector capacity
Ambulance services are just as exposed to the pressures placed on the NHS by an ageing and growing population, and because of the nature of their work, are hit hard by the increasing need for emergency care for patients with increasingly complex conditions.
However it is more difficult to calculate a specific figure to reflect the very real capacity pressures facing the sector. This is mainly due to the recent changes in performance targets for ambulances, which make it difficult to describe how much extra would need to be spent to return the service to good performance against the standard.
Ambulance services are just as exposed to the pressures placed on the NHS by an ageing and growing population, and because of the nature of their work, are hit hard by the increasing need for emergency care for patients with increasingly complex conditions.
While we support the introduction of more clinically led ambulance standards, the new regime may also be creating additional cost pressures by bringing in new targets for low acuity calls. It is still too early to say for sure what the impact of this has been on trusts, however some, particularly those covering large geographies and remote areas, report that the new more rigorous regime has created additional pressure on resources.
Unlike with mental health and community services, where the workforce has very clearly been cut in recent years and needs to be restored, the picture is more complex in the ambulance sector. Overall numbers of ambulance staff, paramedics and support staff have all increased significantly since 2010. The issue is that they have not increased sufficiently to keep pace with demand or changes to their role.
The ambulance workforce is made up of an increasingly diverse group of professions, all playing a role in reducing attendance at emergency departments by giving more treatment in patients homes and elsewhere in the community. This can help reduce the numbers of people being brought to hospital, and the impact of this could be significantly increased if there was a substantial rise in the numbers of advanced and specialist paramedics able to provide this care.
However, over time it will also change the level of acuity among patients being brought to emergency departments, which in turn impacts on the proportion requiring admission. Therefore, calculating and costing the staffing shortfall is difficult to do reliably, especially in a year when the centrally reported performance standards have changed.