The operational ask for 2022/23
The operational ask, set out in the planning guidance and subsequent guidance on elective recovery, requires trusts to balance a number of priorities: to continue to respond to COVID-19 pressures, to tackle long waits across all services and to push forward with the next phase of implementing the NHS long-term plan.
Trust leaders know that many people are waiting longer than they should to access mental and physical health services and are working hard with system partners to help mitigate the risks for patients. The national focus on bringing down the elective care waiting list of 6.3 million (April 2022) does not tell the whole story – there are also increasing pressures on the ambulance sector, and care backlogs across community and mental health services.
While performance against many of the existing waiting time standards has fallen across nearly all metrics, activity levels across services have improved, exceeding pre-pandemic levels in some specialities including mental health, cancer services and diagnostics. These activity gains are a significant achievement, particularly factoring in the complexities and obstacles trusts are facing.
Barriers to improving performance and expanding activity
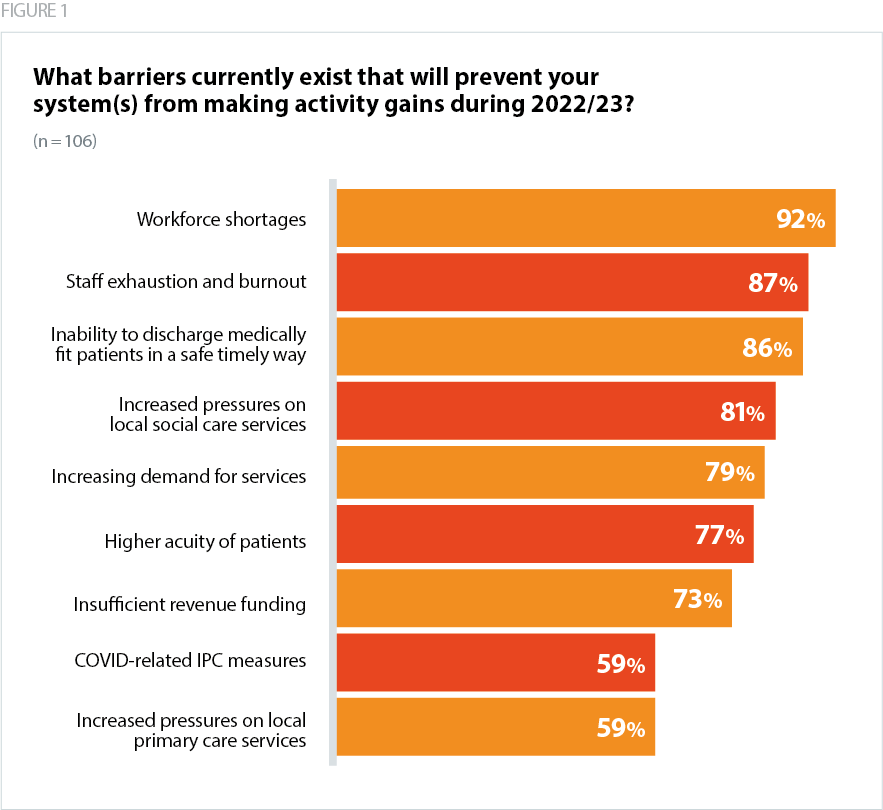
As figure 1 shows, trusts report that barriers to further activity gains include workforce shortages, staff exhaustion and burnout, the inability to discharge medically fit patients in a safe timely way, and increased pressures in social care. Increasing demand for services and higher acuity are also impacting services.
Workforce
- 92% of respondents said persistent workforce shortages are the most significant limiting factor on activity gains in 2022/23.
- 74% of respondents are not confident (42%) or not at all confident (32%) that they will be able to recruit and retain sufficient staff to meet performance and recovery targets in 2022/23. Respondents from mental health and learning disability trusts were most concerned (93% are not confident or not at all confident).
Workforce shortages were a persistent challenge before the pandemic. Despite a positive impact on attracting prospective health care professionals into education, training new staff takes years, and in the last quarter of 2021/22 there were 106,000 vacancies across the NHS, excluding primary care.
Current levels of community prevalence of COVID-19 continue to have a knock-on impact on workforce availability. While staff absences have been decreasing over the spring, they remain high, with an average of 75,226 staff absent from work each day between 7 April and 4 May, 30% of which were COVID-19 related.
In a recent workforce survey, trusts told us that severe workforce shortages, exacerbated by these high sickness absence rates, have resulted in the temporary closure of some wards or services. The results of the latest NHS staff survey similarly reflect an increase in the proportion of staff suffering from work related stress, emotional exhaustion and thinking about quitting the NHS.*
*[The NHS staff survey found 46.8% of staff have felt unwell due to work-related stress in the last 12 months, this is 2.8% higher than 2020 and 8.4% higher than 2017. 38% of staff said work is often or always emotionally exhausting, 34.3% are often or always burnt out due to work, and 31.1% are often or always exhausted at the thought of another day at work.]
Capacity constraints and patient flow across systems
- 86% of survey respondents highlighted difficulties discharging medically fit patients in a safe and timely manner.
- Over 70% of trusts are not confident about their ability to find local solutions and use existing funding streams to ensure the safe and timely discharge of medically fit patients. Many cited more support for social care and domiciliary care as a key solution.
Challenges with patient flow manifest in different ways for different services. For acute hospitals, the inability to discharge a significant proportion of medically fit patients to services in the community, at home or with social care support, means that they do not have available beds for patients arriving by ambulance or via A&E. By way of illustration, on 30 April 2022 there were 20,155 patients who no longer met the criteria to reside in hospital. Of these, 62% remained in hospital on that day.
Consequently, spring 2022 has been one of the most challenging times across the urgent and emergency care pathway. Key indicators such as the length of time it takes to transfer a patient from an ambulance to an emergency department and the number of patients waiting longer than 12 hours in A&E to be admitted following a decision to admit have reached levels never seen before. These blockages at the 'front door' of the NHS are a symptom of system wide capacity constraints across health and social care.
Community trusts and mental health and learning disability trusts also report considerable increases to caseloads and are experiencing similar issues moving patients between services. Capacity constraints have meant that placing mental health patients out of area has also increased, reversing progress made on this issue before the pandemic.
Higher levels of complexity and acuity
- 77% of respondents to our survey said that the higher acuity of patients was impacting their ability to speed up recovery.
Trust leaders are reporting an increase in the complexity and acuity of patients across both mental and physical healthcare services, including within the community. For example, mental health services tell us that they are seeing far greater numbers of children and young people with eating disorders. So, not only are the numbers greater, many of the patients are also more unwell than the equivalent cohort of patients before the pandemic.
When acuity is higher, patients' care needs are more complex, they need more interventions, and are usually in hospital or in contact with community or mental health services for longer. Hospital data from this winter showed increases in the length of stay compared to before the pandemic which trusts have linked anecdotally to increased acuity as well as the challenges with timely discharge explored above.
Elective recovery
In April 2022 NHSE set out new milestones for delivering the elective recovery plan. The ambitions for improving planned and cancer care hinge on increasing surgical capacity through: surgical hubs, transforming diagnostics by creating more community hubs, redesigning outpatient care so it is more personalised, as well as increasing capacity through workforce initiatives, digital innovation and use of the independent sector.
Confidence in meeting targets
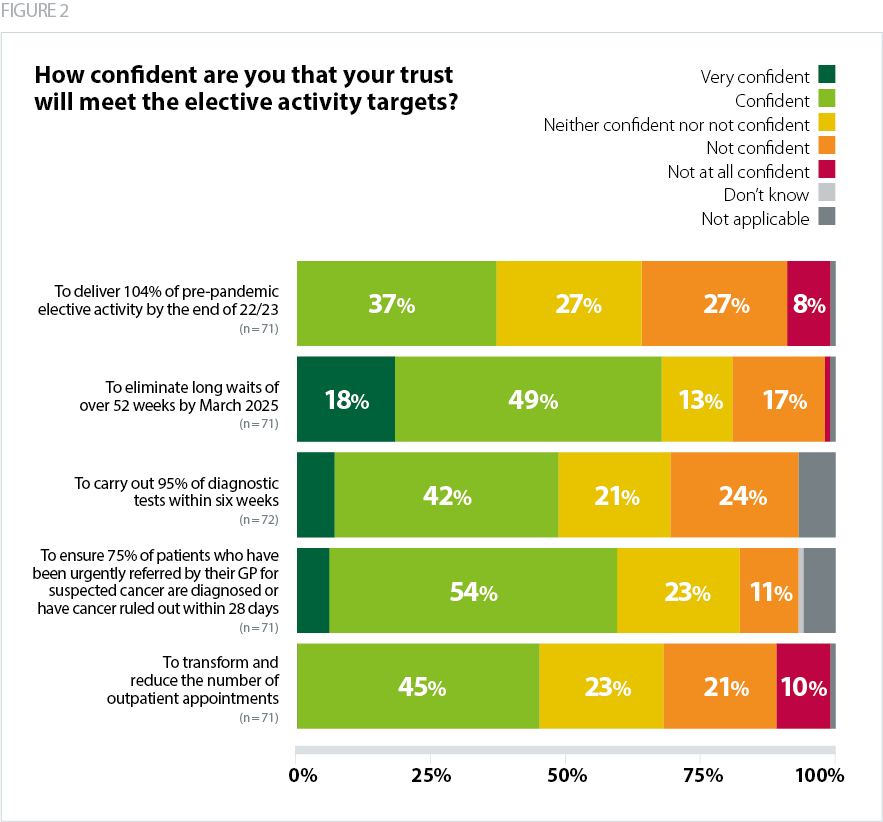
- 67% of respondents who provide elective care said they are very confident or confident that they will be able to eliminate long waits of over 52 weeks by March 2025.
- Only 37% of respondents who provide elective care are confident they will be able to deliver 104% of pre-pandemic elective activity by the end of 22/23.
- 42% of respondents from trusts that provide elective care are not at all confident or not confident that they will deliver their recovery targets to reduce long waits in 2022/23.
With some exceptions due to complexity or patient choice, the majority of trusts are on track to treat all patients waiting over 104 weeks by July 2022. Systems are now turning their focus to eliminating waits over 78 weeks. However, as figure 2 shows, confidence levels in meeting targets for 2022/23 and beyond vary.
Diagnostics and cancer
- Half of respondents (49%) are very confident or confident that their trust will carry out 95% of diagnostic tests within six weeks by March 2024.
- 60% of respondents are very confident or confident that their trust will ensure 75% of patients who have been urgently referred by their GP for suspected cancer are diagnosed or have cancer ruled out within 28 days.
Reducing outpatient appointments
- 45% of respondents are confident that their trust will reduce the number of outpatient appointments.
Respondents told us they are optimistic that their trust can deliver this over the next three to five years but not at the pace the plan requires. Some trusts highlighted the importance of follow-up appointments in closing off patient pathways, and that the transition to reduced appointments needs to be realistic. Respondents also stressed that the target to reduce outpatient appointments needs to be appropriate to the care pathway, particularly for specialist services where treatments are primarily outpatient based.
Balancing elective recovery with the wider care backlog
- 79% of respondents said that increasing demand for services was preventing their system from making activity gains during 2022/23.
- Half of respondents (51%) are not confident or not at all confident that their system will deliver its recovery targets to reduce long waits across mental health services.
Trust leaders report increasing pressures on mental health providers, with recent data showing there are more people in contact with services than ever before, and a significant level of unmet need. Community trusts are also facing an increasing care backlog with estimates that almost a million were waiting for care at the end of 2021. Respondents highlighted the fact that elective recovery targets and pathway changes require support from primary care and community services. Community providers have also asked for similar flexibilities to colleagues in the acute sector, including a support package, and 'air cover' from NHS England to cut waiting lists to tackle health inequalities as well as reduce waiting times.