- Trust boards have a critical role to play in driving change on race equality and health inequalities - both within their organisations, as well as contributing to wider system efforts. Trusts are at different stages of rising to this challenge. Boards' responses to addressing health inequalities vary substantially, informed by the geographic and socioeconomic context they operate within, as well as the types of services they provide, and the relationship they may hold with their community as a result.
- There are high levels of board commitment and strategic emphasis on tackling health inequalities. However confidence was lower when it came to the arrangements trust boards have made to put this into practice, including action on preventative programmes, and digital inclusion.
- Trust leaders describe a number of barriers to progress. The majority say that wider system pressures and operational challenges act as a hindrance to their work on health inequalities, and access to data about health inequalities within their trust and across the wider system is also a challenge.
- A nationally coordinated approach to addressing these barriers will be needed, but trusts also express a commitment to move forward from board-level conversations to begin embedding action on health inequalities as 'core business'. Two key enablers include robust data analysis, enabling them to prioritise and simplify action on health inequalities, as well as harnessing the insights and skills of frontline staff to increase capacity across the trust.
- Health inequalities do not begin or end with individual trusts. Trust leaders recognise that while they will lead much of the work to address healthcare inequalities, the broader health inequalities people face as a result of the wider determinants of health will require a system-wide effort if they are to be fully addressed.
- There is an important role for trust boards in building a culture of equity into services which recognises that to achieve the same outcome, some people need different routes to access services. Trusts highlight a need for compassionate conversations about how to address health inequalities in ways which avoid placing blame, but rather facilitate clinicians to work together to design solutions which improve access and narrow health inequalities where they can be found.
- Trusts need an enabling regulatory environment to meet their objectives to reduce health inequalities, and to effectively work with their system partners to improve outcomes across the wider determinants of health. To cement a long-term commitment to improving health inequalities as part of their 'day-to-day business', trusts will need a supportive infrastructure which measures and rewards progress on health inequalities as much as it does good operational and financial performance.
High levels of commitment at board level, despite challenges
The survey looked at the confidence trust leaders have in the board level arrangements they have in place to address health inequalities. This identified specific areas of strength and areas that need further development.
Board-level commitment and a strategic emphasis on tackling health inequalities is high, with two thirds of respondents (65%) saying they are confident that their board has effective leadership commitment and governance in place to address health inequalities. However, confidence was lower when it came to the arrangements trust boards have made to put this into practice. Around half of respondents felt confident in their board’s arrangements to reduce inequalities in their own workforce (55%) and to work collaboratively in their ICSs to address systemwide inequalities (47%).
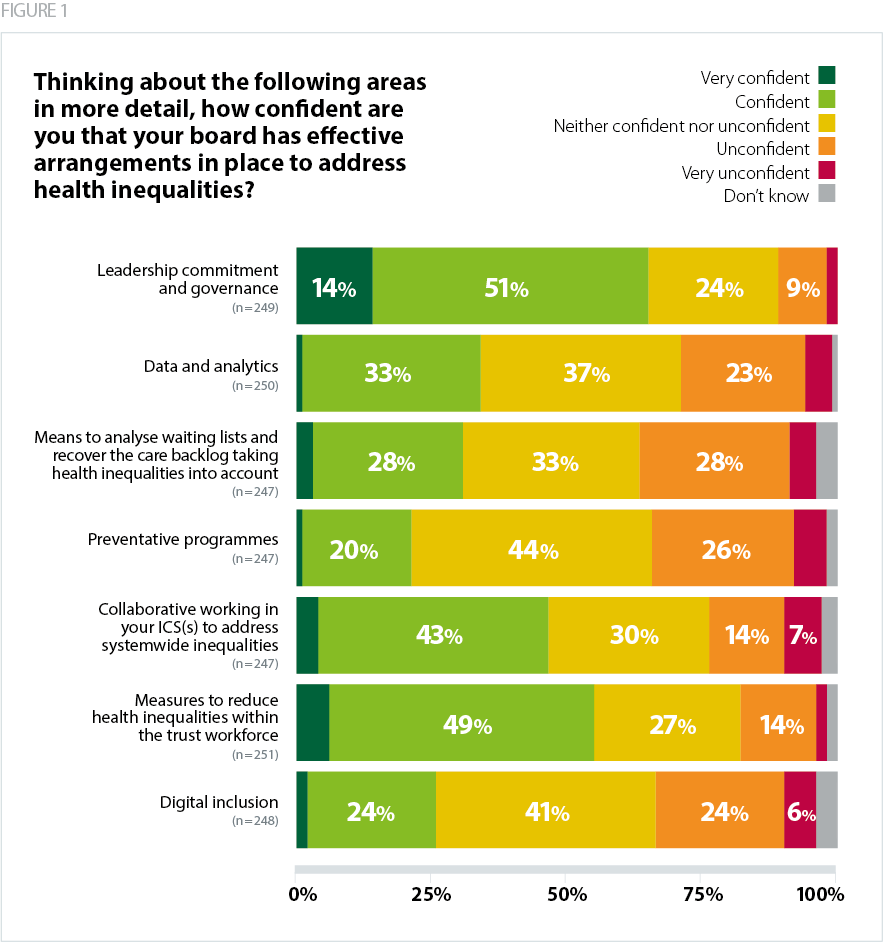
However, trusts also describe a lower level of confidence across a number of measures. A fifth (21%) felt confident in their board level arrangements on preventative programmes, around a quarter (26%) expressed confidence regarding their trust's work on digital inclusion, while a third (34%) said they were confident about data and analytics on health inequalities. (Figure 1).
There is variation between trust sectors. For example, while acute trusts are less confident in their measures to address inequalities in their workforce, they are more likely than average to describe themselves as confident in their means to analyse waiting lists and recover the care backlog taking health inequalities into account. Conversely, community trusts describe lower confidence in reducing the care backlog with health inequalities in mind, but are more confident than the trust sector average in their collaborative working to reduce health inequalities across the ICS, and preventative programmes. Mental health trusts are more confident on digital inclusion, and ambulance trusts describe higher confidence in measures to reduce health inequalities within the trust workforce.
It is perhaps unsurprising that trusts rated their leadership commitment and governance arrangements around health inequalities more highly than operational measures. Trust leaders are clear that in order to effectively move the dial on health inequalities, board-level leadership and shared commitment to improvement is a key building block of an effective trust level response. Even for those trusts which are only recently beginning to consider how they best respond to health inequalities; the leadership and governance arrangements are an important starting point.
However, we also know that two key aspects of concrete action on health inequalities are robust use of data and analytics, and strengthening preventative action for groups at greater risk of poor outcomes due to structural inequalities. They have been identified as key national priorities, so the fact they have been identified as areas of difficulty points to a need for targeted support to enable boards to carve out time and resource to address these areas.
The data we have is often derived from a mix of different digital and paper based systems; an integrated digitally based system for the trust would provide real time information, making evidenced based decisions more timely.
Chair
In an environment where trusts are balancing multiple priorities, including reducing the care backlog, managing staff shortages, and planning how they will meet a tough financial ask, trust boards must prioritise key areas for initial, focused action. With time and effort boards will be seeking to move from analysis to action and begin to focus their attention more closely on specific programmes which can help drive meaningful improvement in access, experience and outcomes for people facing health inequalities.
I think this is about us finding a way to dedicate time to it.