The workforce gap has developed in plain sight. The fact that such a large problem has developed in this way suggests that NHS strategy, planning, and policy making structure and approach in this area is flawed and needs urgent review.
This has been widely recognised. In June 2016 the House of Commons health select committee in its report on managing clinical workforce supply, concluded that:
“The Department of Health and its arm’s-length bodies have provided ineffective leadership and support, giving trusts conflicting messages about how to balance safe staffing with the need to make efficiency savings. In addition, overseas recruitment and return-to-practice initiatives, which could help address current shortfalls, have been poorly coordinated. The national bodies need to get a better grip on the supply of clinical staff in order to address current and future workforce pressures.”
More recently, the House of Lords select committee on the long-term sustainability of the NHS said in its report of April 2017:
“We are concerned by the absence of any comprehensive national long-term strategy to secure the appropriately skilled, well-trained and committed workforce that the health and care system will need over the next 10-15 years. In our view this represents the biggest internal threat to the sustainability of the NHS. Much of the work being carried out to reshape the workforce is fragmented across different bodies with little strategic direction from the Department of Health.”
And in the run up to the recent June 2017 general election, the independent think tank The Health Foundation, in its pre-election briefing, concluded:
“The NHS still has no overarching strategy for its workforce. Piecemeal policymaking, however well intentioned any individual initiative might be, is not serving the NHS well.
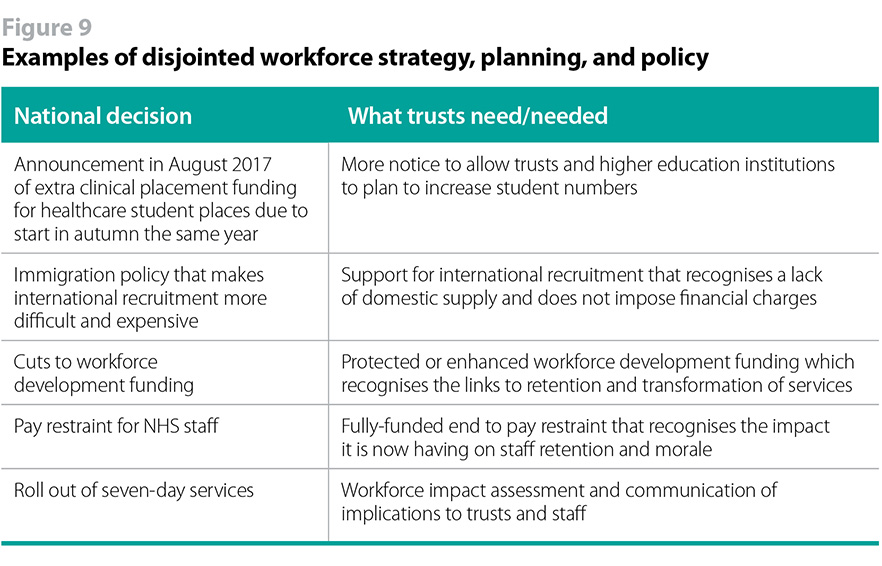
Yet, the Department of Health and the NHS national bodies have been slow to respond and the action that has been taken has been piecemeal, creating confusion among provider trusts and staff as to what the overall strategy is and a lack of confidence that the array of initiatives that have been announced will succeed in closing the workforce gap. According to our recent survey, 90% of trust chairs and chief executives are worried or very worried about whether the Department of Health and the NHS national bodies’ approach to workforce strategy, planning, and policy will support their trust to recruit and retain the staff they need. This is deeply concerning.
There has also been an over-focus on the pipeline of future staff. The supply of future staff is essential. But too often issues and actions that need to be addressed in the short term have been overlooked, with the NHS expected to hang tough until the longer-term actions come to fruition. More energy and money needs to focus on shorter-term ways of mitigating the workforce gap.
A coherent approach
There has been a lack of joined-up thinking and action due to the fragmentation of responsibility for workforce strategy, planning, and policy across the national bodies within the Health and Social Care Act landscape. While the Department of Health is ultimately accountable, responsibility for workforce strategy and policy is shared across the various NHS national bodies.
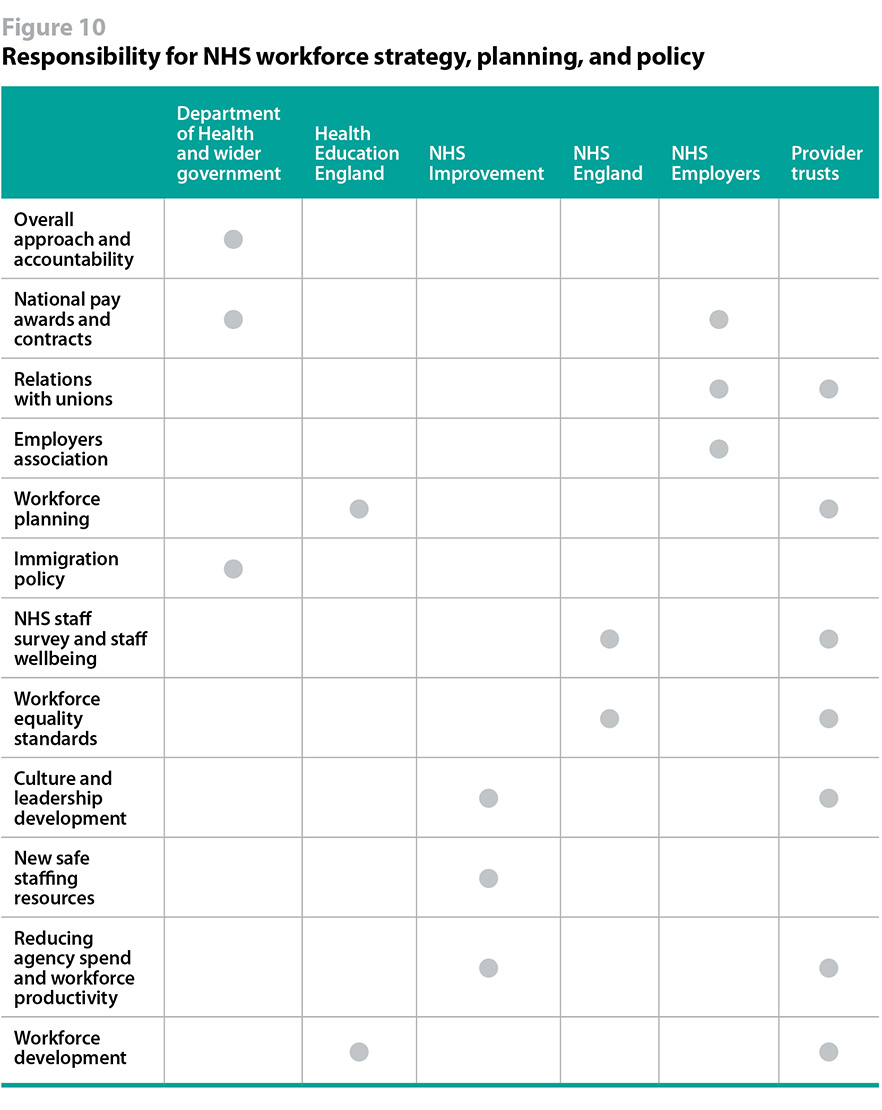
The Department of Health, recognising this fragmentation, and the need for a more coordinated approach, has established a ministerial board on workforce. It brings together senior leaders from the NHS national bodies. While it is not in itself a problem, and is to some extent inevitable, that the various national bodies have workforce functions to fulfil, it is a problem when there is no overall agreement on what they want to achieve and how they will exercise their respective functions to do so. The ministerial board has an opportunity to develop and communicate a coherent and credible workforce strategy with plans to close the workforce gap.
If the ministerial board is to be the key forum overseeing and coordinating NHS workforce strategy, planning and policy, it needs to communicate effectively about its work, seek input from a wide range of opinion, be transparent about its work programme and be seen to engage effectively with provider trust leaders. While NHS Employers membership of the board is welcome, this is not a substitute for the above.
A credible approach
The piecemeal and lack of overall approach to workforce strategy and policy at the national level also reflects the political difficulty of acknowledging and addressing the funding gap linked to the workforce gap. In order to ensure sufficient supply the training of future staff must be adequately funded. And, crucially, trusts must also be adequately funded to employ the levels of staff that they need to deliver high-quality care.
The migration advisory committee made this point in its conclusion to its partial review of the shortage occupation list in respect of nurses in March 2016:
“It is clear to us that the current shortage of nurses is largely of the health, care and independent sectors’ own making. The sector’s failed to train enough nurses or failed to make provision to train their own nurses should the supply of publicly funded nurses fail. They have taken either no or insufficient account of the needs of other sectors when making their planning assumptions. They restricted pay growth. They have complex institutional structures, which blur the decision-making process and lead, among other things, to poor information and data making it difficult for them (and us) to understand and respond meaningfully to labour shortages. They did not learn the lessons from the late 1990s/early 2000s when a similar shortage (and reliance on foreign nurses) occurred. Almost all of these issues relate to, and are caused by, a desire to save money. But this is a choice, not a fixed fact. The government could invest more resource if it wanted to.”
Decisions at the national level have often been swayed by resourcing decisions. In the case of pay restraint this is very clear. But it is also seen in the cutting of the workforce development budget at a time when the NHS is attempting to transform services.
A failure to face up to the funding gap at the national level also trickles down through the system to decisions made by provider trusts. As the Health Foundation put it in its report Staffing matters, funding counts:
“Effectively aligning staffing objectives with funding streams is also vital, but has often not been the case. This is not a direct result of technical shortcomings in the workforce planning approach (although sometimes ‘poor workforce planning’ has been a convenient excuse) but relates more to poor strategic coordination and conflicting political, funding and planning objectives and cycles.”
When preparing workforce plans, provider trusts are required to forecast their future demand for staff. While they may know how many staff they need to deliver high-quality care for patients, they will also know how much money they have been allocated to deliver services and will be expected to ensure they do not demand and employ more staff than they can afford. It would not be surprising therefore if some trusts submitted ‘affordability adjusted’ demand forecasts for clinical staff. To the extent that national-level forecasts of demand for staff are developed on a bottom-up basis, this can mean they understate the staffing levels that will be needed.
Efforts to close the workforce gap
The Department of Health and the NHS national bodies are taking action. There has been a somewhat bewildering array of announcements. But so far this has appeared piecemeal and it is not clear that the various initiatives will add up to the answer to the workforce gap the NHS faces. It doesn’t help that, as of October 2017, the 2017/18 workforce plan for England has still not been published and we are halfway through the financial year.
As one trust leader put it: “Our staff are really our greatest asset and definitely go the extra mile for our patients but consistent workforce availability is vital to safety and quality and drives the money. It feels like there is no national focus or coherent plan. This is not something each trust can resolve on its own”.
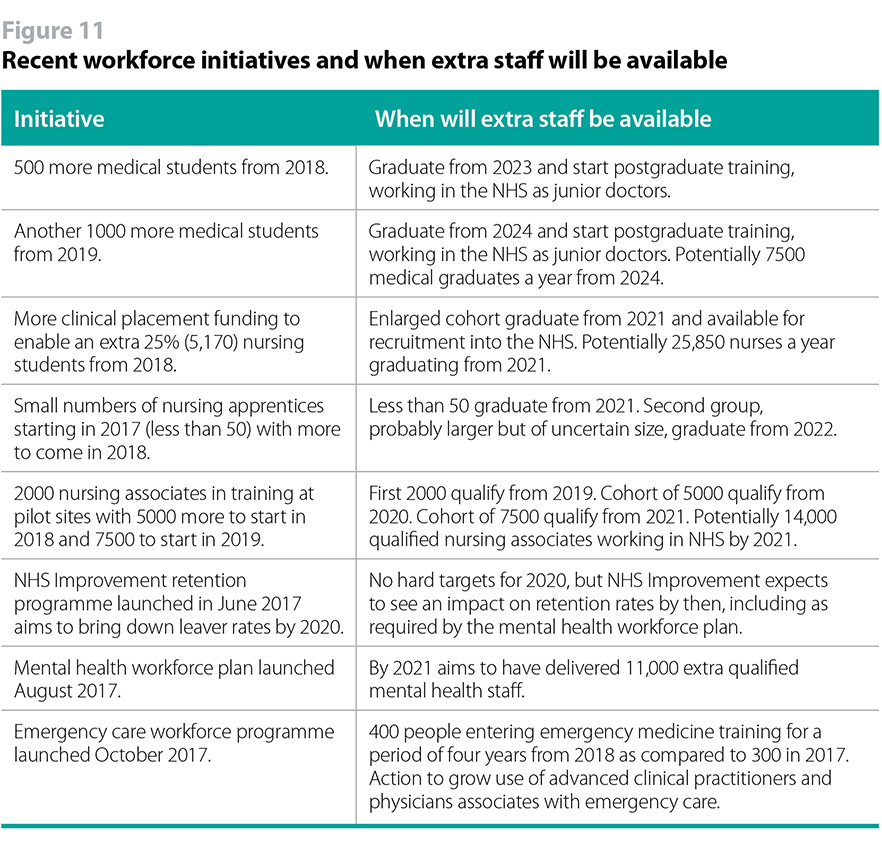
As figure 11 illustrates, many of the initiatives will also take several years to bear fruit, whereas the NHS also needs action with short-term payoffs to address the workforce gap in the meantime, including international recruitment and decisions on issues that affect recruitment and retention.
As another trust leader put it: “Extra training places resulting in more staff in three or five years does not solve the crisis.”
Empowering provider trusts to lead on workforce
What our research and discussions with trusts has shown is that any workforce strategy will only work if there is a coherent and credible planning and policy making structure that links and aligns what needs to be done at national level, regional level, and at an individual institutional level.
The current structure and approach clearly needs review. Trusts have lost confidence in current arrangements and there is a question as to whether a radical rethink is necessary.
Greater national coherence and credibility is part of the answer. But there should also be an important debate about what should be better done at the regional and institutional level. We are already seeing trusts and groups of trusts beginning to take greater responsibility for solving their current challenges and closing the workforce gap. But while they are increasingly taking on responsibility where national arrangements are seen to have fallen short, they have not yet been given the resources or developed the capability to support them to do this job effectively on a large scale.
There is a strong argument that appropriately resourcing trusts to take on greater workforce responsibilities, within STPS or other aggregated footprints, is the right direction of travel and needs to be encouraged and accelerated. Yet it raises big questions:
- What is best done at national, regional, and institutional level?
- If more is to be done below national level, what resources should be devolved and what should the regional or sub-regional footprint and infrastructure look like?
- What sub-national capability will need to be developed?
These are big questions but we think there should be a review to test the idea that the NHS should genuinely devolve more responsibility and resources for more workforce issues to the sub-national level. For example, there could be work on workforce planning and distribution of training budgets at the regional level, with trusts working closely with higher education institutions, while there may also be opportunities to address issues affecting staff wellbeing and recruitment and retention such as affordable housing for NHS staff. There is at present little appetite for regional pay arrangements. It is vital that provider trust leaders are fully involved in the review. Changes of this magnitude would need to be carefully thought through.
Fragmented responsibility – what needs to happen
In the medium term, the Department of Health and the NHS national bodies should:
- develop and communicate a coherent and credible strategy for the health and social care workforce, setting out what they think the future workforce needs to look like given the Five-year forward view, STPs, and new care models and what will be done, by who, and by when to at the national level to develop that workforce;
- ensure the existing ministerial board on workforce is recognised as the forum to coordinate and own this strategy, in collaboration with provider trusts and other stakeholders. It needs to communicate effectively about its work, seek input from a wide range of opinion, be transparent about its work programme and be seen to engage effectively with provider trust leaders;
- develop a measurable plan with timetables to grow the domestic supply of clinical staff, taking account of relevant factors such as changes to the funding of healthcare education, the apprenticeship levy and targets, the expansion of nursing, and the recent workforce plans for mental health and emergency care workforces. This plan will link to and support the strategy;
- take action to ensure there is an agreed and publicly accessible source of timely and accurate national-level, regional, and trust-specific data for key workforce data such as vacancy rates and leaver rates;
- provide greater transparency of its workforce planning insight and data, for example timely publication of national and regional demand and supply forecasts for the different staff groups, together with the assumptions and any funding constraints that underpin them;
- work with provider trusts at the sub-national level – for example, devolved, groups of STPs, or STP-level as appropriate – to support the delivery of locally-owned workforce strategies and plans that support service transformation through provision of timely and tailored workforce planning insight and data.
For the longer term, the Department of Health and the NHS national bodies should:
- work with provider trusts and other stakeholders to explore the opportunities and risks of devolving elements of workforce responsibility and funding – for example medical education and training commissioning, distribution of clinical placement funding. This could be at devolved, groups of STPs, or STP level;
- develop the capability and capacity of provider trusts to take on this greater role, building on the lessons from the original plans for local education and training boards with strong provider leadership. The return on this investment could be a more engaged, responsive, and productive workforce;
- build and value local leadership and autonomy as crucial for the success of STPs and new care models.